Studies of the connection between migration and health are often unsatisfactory because of the lack of explicitly-formulated explanatory models.
Explaining The Relationship Between Migration and Health
/ 8 Minuten zu lesen
Patients at a walk-in clinic for illegal migrants in Berlin. (© picture-alliance/dpa)
Even in the field of epidemiology, interest in including migrants in epidemiological studies has awoken only in recent years.
The "healthy migrant" phenomenon
Compared with the majority population, many migrants are socially and economically disadvantaged, and for that reason it might be expected that their health should also be measurably worse. Social epidemiology tells us that a lower socio-economic status raises the risk of disease and premature death. Adult migrants from many countries of origin who migrate to European countries or the USA, however, present lower mortality figures than the non-migrant majority population in the host countries. In some age groups their mortality can be up to 50% lower than in the majority population.
| Mortality of migrants relative to the population in the destination country | |||||
| Origin | Destination country | Data source | Measure | Relative risk Men - Women | Reference |
| China | Canada | Canadian Mortality Database | RR | 0,55 - 0,63 | Sheth et al. 1999 |
| Mexico | USA | National Longitudinal Mortality Study | HR | 0,57 - 0,60 | Abraido-Lanza et al. 1999 |
| Vietnam | England | National Health Service Register | SMR | 0,64 - 0,56 | Swerdlow 1991 |
| Southern Europe* | Germany | German Socio-Economic Panel (SOEP) | RR | 0,68 | Razum et al. 2006 |
| Former. USSR** | Germany (North Rhine-Westphalia) | Population and cause of death statistics | SMR | 0,89 - 0,81 | Ronellenfitsch et al. 2006 |
| esp. Latin America, Asia | USA | National mortality data | RR | 0,77 - 0,84 | Singh & Hiatt 2006 |
| *"Guest worker"-recruitment countries in the Mediterranean area(Turkey, Yugoslavia, Italy, Spain, Portugal); men and women combined **Ethnic Germans (Aussiedler/Spätaussiedler) RR: Relative Risk; HR: Hazard Ratio; SMR: Standardised Mortality Ratio. These measures indicate the mortality of migrants relative to the population of the destination country. Example: RR = 0,55: male Chinese immigrants in Canada have a mortality factor of 0.55 in relation to Canadian males. This equates to a lower mortality (calculated as 100 - 0,55 x 100). | |||||
| Source: Razum (2006) | |||||
This migrant mortality advantage observed in many data records is referred to in literature as the "healthy migrant effect", or the "phenomenon of the healthy migrant". It is unlikely that this is solely a selection effect among migrants. It is true that migrants are often especially healthy people. However, their health advantage should be apparent in relation to the population of the country from which they originate and not necessarily in relation to the population of the country to which they have migrated. In addition, the advantage is often still apparent years after migration, despite the unfavourable socio-economic conditions under which migrants often live. In view of the inverse association between socio-economic status and mortality, the healthy migrant effect represents a paradox.
Distortions
Artefacts or distortions in the available data are repeatedly cited as explanations for the apparent health advantages or lower mortality of migrants.
Social support
Better "social support" among the migrant population than the majority population
Migration as a health transition
The populations of poorer and richer countries are exposed to different factors that affect their health during their lifetime. Global differences in hygiene conditions or nutrition are examples of this. Anyone who migrates across national and also economic boundaries has, for this reason alone, a different risk of chronic disease than the non-migrant population in the country of immigration. This results in apparent paradoxes with regard to chronic disease among migrants.
To resolve these paradoxes it is possible to interpret migration from poorer countries to richer ones as a "health transition". The expression "health transition" is normally understood to mean the transition within a society from high mortality, primarily caused by infectious diseases as well as maternal and infant mortality, to a lower mortality, primarily caused by non-communicable, chronic diseases.
therapeutic components, i.e. better prevention and treatment options for things like infectious diseases
risk factor components, e.g. protection from disease due to the provision of clean drinking water, and also from new risks caused by things like smoking, poor nutrition and a lack of exercise.
A health transition towards chronic disease is proceeding worldwide but at different speeds. Many of the – poorer – countries of migrant origin are still at an earlier stage compared with rich, developed countries such as Germany. If people migrate from a poor country to Germany, the rate at which they acquire new diseases and the rate of death change, occurring at different speeds depending on the type of disease:
The mortality of migrants from treatable infectious diseases and also maternal mortality (still high in many countries of origin) falls rapidly towards the level of the population of the country of immigration – in accordance with the "therapeutic" components of the health transition.
New diseases and mortality among migrants from ischaemic heart disease (heart attack), the most common cause of death in Germany, remain initially on a low level, e.g. that of a country of origin in southern Europe. This is attributable to the mostly long latency period between the escalation of the risk factors and the occurrence of disease. First-generation immigrants can therefore still have a lower risk of heart attack and mortality than the population of the country of immigration many years after migration.
With increasing length of residence – or in subsequent generations that grow up in the country of immigration – migrants adjust to the "Western" lifestyle. With time, this increases their risk of a heart attack
The increased risk of new, lifestyle-related diseases is in addition to the increased risks to migrants of other chronic diseases listed above. Examples include stomach cancer and stroke. These occur in large numbers in people who have spent their childhood in poverty and poor hygiene conditions.
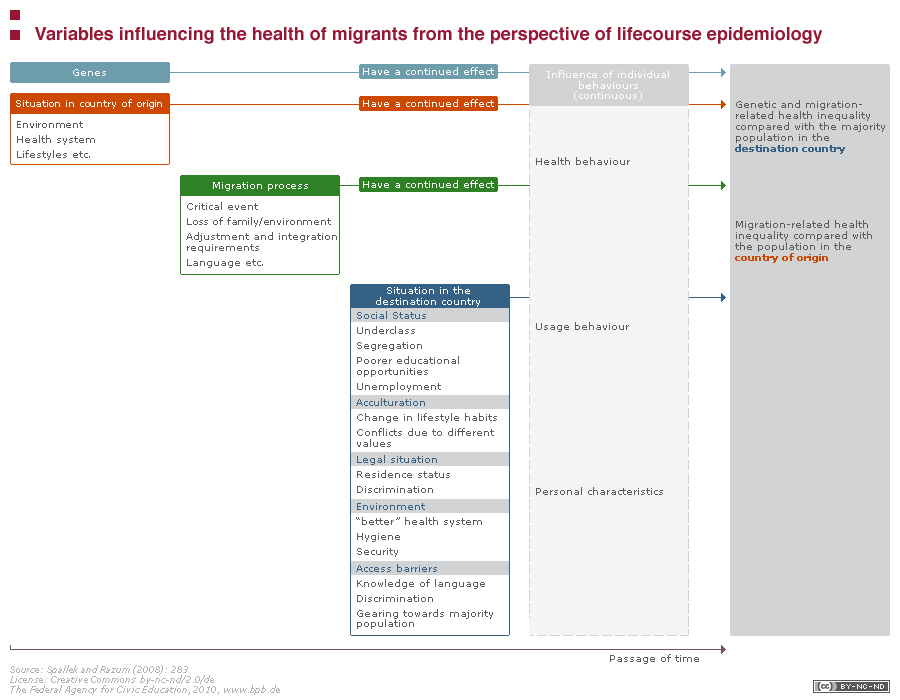
Migration and lifecourse epidemiology
Migrants have often been exposed to different experiences during their lives than those of the non-migrant majority population, especially during childhood in their country of origin. This can lead to unexpectedly different patterns in the occurrence of chronic disease. For some chronic diseases the risk of occurrence in later life – after a long period of latency – is already determined by exposure in early or very early childhood. This makes it necessary to study the entire lifecourse of migrants in order to be able to understand the pattern of their chronic diseases and their mortality. A snapshot at a time after migration is not sufficient. What is more necessary is a lifecourse epidemiology, in other words an epidemiology that factors in exposure throughout the person´s life.
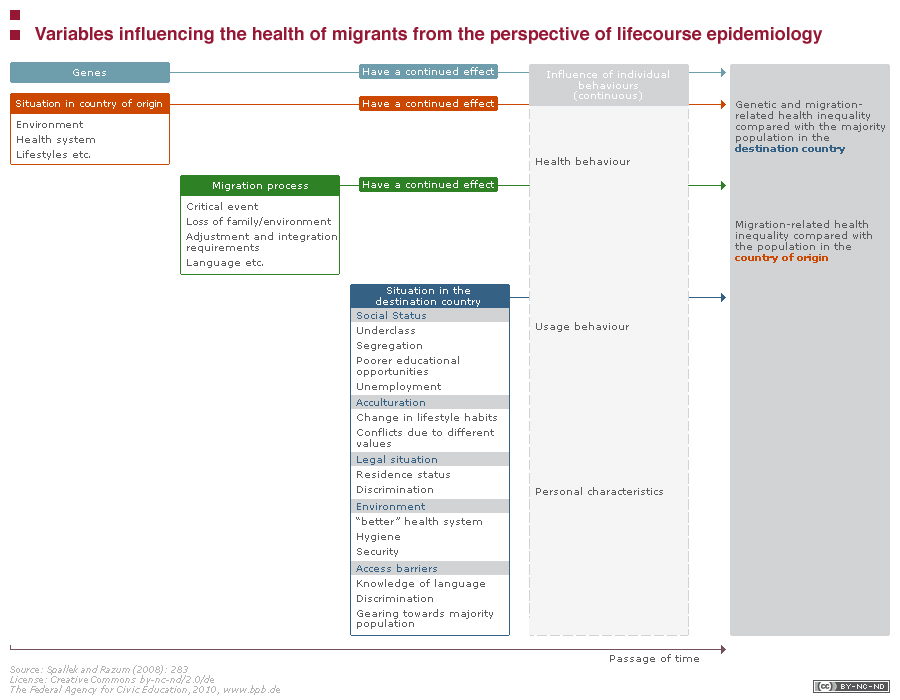{kind=link}
Variables influencing the health of migrants from the perspective of lifecourse epidemiology (bpb) Lizenz: cc by-nc-nd/2.0/de
- Als JPG herunterladen (173.5kB)
{kind=link}
Variables influencing the health of migrants from the perspective of lifecourse epidemiology (bpb) Lizenz: cc by-nc-nd/2.0/de
- Als JPG herunterladen (173.5kB)
In studies on the health of migrants – and thus also in the development of an explanatory model – it is difficult to identify suitable control groups. The differences, for example in the mortality between male and female migrants on the one hand and the majority population on the other, result in part from factors relating to their lives in the country of origin. Anyone migrating to Germany from a southern country bordering the Mediterranean initially brings with them the cardiac mortality associated with that country – far lower than that of the German population. Due to the long latency periods between exposure to risk and disease, this advantage is retained even where there is socio-economic disadvantage. If we wish to differentiate between genetic predisposition and lifestyle influences, then comparison with the population in the country of origin is particularly meaningful. If, by contrast, we wish to make observations on access to health care, comparisons with the population in the migrants´ country of destination are sensible.